NOLO (No One Left Out) Project
Our Story
There is an urgent need to have a population approach to the problems of poor mental health. Health professionals must go into the community as a matter of public health concern and help deal with the problem of poor mental health, just like the approach to contain contagious diseases like polio or HIV/AIDS. In our daily practice as professionals, we meet clients of school-going age who need intervention for poor school performance. We meet those who have developed mental disorders because of a probable psychosocial problem. We also meet those with special needs who call for help.
This call for help may include.
- Support to help their wards integrate into the regular school system.
- Need for medication and medication management.
- There is a need for human resource and capacity building in utilizing behavior modification models in helping children with special needs.
- There is a need to beef up the capacity of teachers and schools to be able to run the inclusive education system.
We can trace how divorce and its fallouts affect children’s school performance. Depression in women during and after pregnancy can have dire consequences on the development of children and the marriage.
We see clearly how poor/low self-esteem, a silent fuel, is underpinning many mental illnesses and poor well-being and its long-term effects on performance. Performing poorly in school is associated with the inability to hold a job, achieve one’s dreams, being caught up in deviant behavior, and risking incarceration or imprisonment for a crime.
Those who get to know someone who can identify the cause of the problem and knows where help is and how to get help. Even so, early intervention is key. There is an urgent need to reach out to our children, leave the comfort of our workplaces from time to time, and reach out to the public. Go to the people in the communities.
Why is it important to target children & young adults?
The majority of mental illness starts in the period of adolescence and early adulthood – at a critical time of development. Poor mental health has the potential to end it all for the hope of countries and our children. Usually, it is silent, and the sufferers hardly talk about it. They may not even know what it is they are experiencing and who and where to seek help.
In 2017, 12.8% of 5-19-year-olds (1.25 million individuals) in England experienced at least one mental disorder [1]
In Ghana, the Prevalence of mental disorders among primary school children and adolescents is 7.25% [2]
[1] (England national survey) (NHSD, 2018a)
[2] Kwabena Kusi-Mensah et al., J Child Adolesc Ment Health. 2019 Dec.
In the Kwabena Kusi-Mensah et al. study, it is cited that the prevalence of Children and Adolescent Mental Health Disorders (CAMHD) was higher in public schools (11.6%) than private schools. This finding had a predictive
relationship with academic achievement, which enforces the need to address the causes of poor school performance to stem the tide.
Some of the mental disorders identified are
- Depression
- ADHD (Attention Deficit Hyperactivity Disorder)
- Intellectual disability
- Conduct disorder
- Seizure disorder
Why is it important to target children and young adults?
Levels of emotional difficulties in girls in secondary schools in England also increased between 2009 and 2014 (cross-sectional studies) (Fink et al., 2015). Among 17-19-year-olds, girls were more than twice as likely to have a mental disorder than boys (23.9%). The annual incidence of self-harm in 13-16-year-old girls increased by 68% between 2011 and 2014 (England population cohort study) (Morgan et al., 2017a).
Lack of social inclusion: Participation among 11-19 year olds (England national survey) (NHSD, 2018a) in school clubs was lower in those with mental disorders (65.9%) than those without disorders (78.6%).
Regarding clubs outside school, participation was lower in those with mental disorders (51.5%) than those without disorders (62.4%).
Antisocial and offending behavior, crime (British and Brazilian cohort studies) (Murray et al., 2015), and violence. (Ferguson et al., 2005/New Zealand cohort study; SCMH, 2009; Murray et al., 2015).
Bullying: Young people aged 11-19 with mental disorder were more likely to bully others in the past year (28.3%) than those without mental disorder (14.0%) and more likely to be bullied in the past year (59.1%) compared to those without mental disorder (32.7%) (England national survey) (NHSD, 2018a).
There is a higher likelihood of seeking identity in bad company or behaviors or escaping the mental health challenges through the use of hard drugs only to move from frying pan to fire.
Why is it important to target children and young adults?
Lower well-being (England national survey) (NHSD, 2018a)
- Mental wellbeing was lower in 11–19-year-olds with a mental disorder (43.1) compared to those without a mental disorder (53.0).
- Well-being levels varied by disorder and were higher for neurodevelopmental disorder (48.4) and lowest for emotional disorder (41.8).
- High self-esteem was five times less common in 11–19-year-olds with mental disorders (5.2%) compared to those without mental disorders (25.1%). High self-esteem levels varied by disorder from 14.1% for neurodevelopmental disorder to 3.7%.
For all that children and young adults may be going through…….
For all the dysfunction and divorce going on……..
For all the psychosocial problems they encounter……..
For all the problems women face during and after pregnancy…….
IS A SILENT CANKER
It eats up vulnerable people till the day comes when the brain and body can no longer compensate for all the negative emotions, thoughts, perceptions and feelings and behaviour………….
What do we do about the problem?
The problem of mental health is like an octopus, it is hydra-headed. Where do we tackle the problem from to make the most impact?
Where will minimal resources yield maximum results?
- Primary public mental health
- Awareness creation & knowledge sharing.
- Early intervention.
- Preventive measures.
Since in the early stages of poor mental health, the signs and symptoms are not easily seen or people find it difficult to talk about, we needed an indicator everyone can relate to.
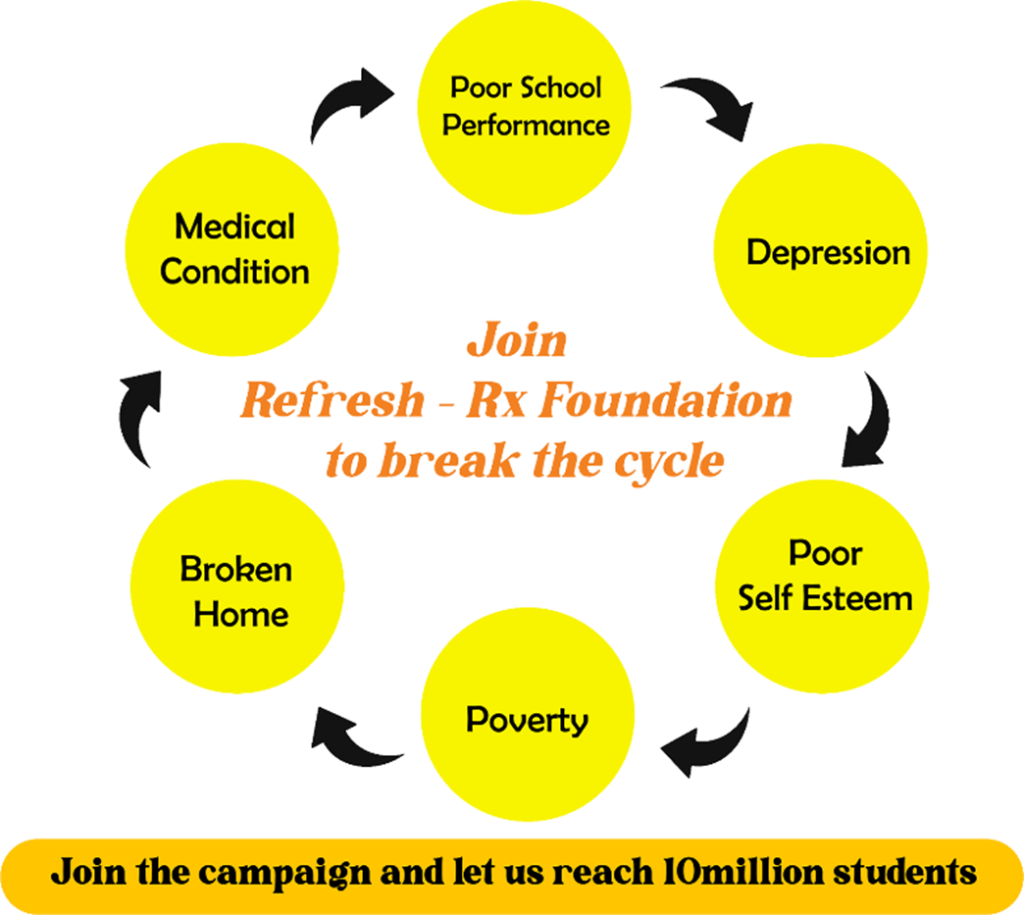
Poor school performance is the tip of the iceberg and itself can also cause poor mental health, low self-esteem, behavior problems, drug abuse, relationship problems, and low productivity. Worse, it is the fuel that drives the wheels of the vicious cycle of poverty, and poverty can cause mental illness.
Why use school performance as an indicator & the turn key?
The current survey by the security agency reveals Ghanaians spend about five hours on social media, mainly involved in pornography and betting.
Is anybody looking at the underlying identity problem?
‘No One Left Out’ (NOLO) project seeks to raise awareness about the causes of poor school performance (PSP) and the interventions accessible to parents, students, and teachers through a public awareness campaign.
We wish to address the ‘Kofibaboni’ myth of defining certain groups of persons as unable to fully realize their potential.
Medical disorders such as autism, attention deficit hyperactivity disorder (ADHD), epilepsy, cerebral palsy, and intellectual disabilities are some causes of PSP.
Problems with handwriting, reading, speech, vision, and hearing; adequate nutrition; traumatic events; conflicts in the family; dysfunctional homes; poor self-esteem; and other psychosocial factors all contribute to poor school performance. It is not always the case that the child is not intelligent.
What do we want to achieve with the NOLO project?
Our goal for the awareness campaign is to make referral of children with poor school performance to a pediatrician common knowledge to all Ghanaians of all walks of life. Our first five-year plan is to reach ten (10) million individuals with our awareness campaign and assist one million Ghanaian school children and a hundred teachers through our on-site intervention programs. The project’s intervention arm aims to directly adopt schools in Ghana.
What will we do to achieve our target?
The awareness campaign will be conducted via in-person visits to schools, churches, and mosques and the use of all social media channels.
The on-site intervention program will be started with a baseline screening of pupils/students for possible causes of poor school performance.
Screening will cover eye and ear exams, reading skills, handwriting, and psychosocial and mental health screening.
Appropriate referral to pertinent health experts such as speech therapists, ear, nose, and throat therapists, occupational therapists, clinical psychologists, pediatricians, public health experts, and pharmacists as and when needed.
A capacity-building workshop will be organized for teachers to enable them to support students with PSP. Attention will be given to the psychosocial needs of students.
Studies have shown that self-esteem, mental health, and literacy are three (3) factors critical for a student’s wellness in life and school performance.
Therefore, a self-esteem and literacy club will be set up in the schools to aid students in improving their interpersonal and intrapersonal relationships, impacting their total ability to thrive in life.